Surgeons Preserve Patients’ Hearing with Innovative Brainstem Implant
FDA-approved device helps patients with neurofibromatosis type 2
Published Date
Article Content
Patients with rare brain tumors on the auditory nerve now have an option to prevent complete deafness at UC San Diego Health. The device, called an auditory brainstem implant or ABI, fits behind the ear and connects directly to the brainstem. The device enables patients with neurofibromatosis type 2 (NF2) who develop bilateral hearing nerve tumors to be aware of environmental sounds, such as a door opening, a phone ringing or a car approaching.
“An auditory brainstem implant can have a profoundly positive impact on a patient’s quality of life,” said Marc Schwartz, MD, neurosurgeon at UC San Diego Health. “The device helps patients to perceive sound and communicate more effectively through lip reading. It was designed for patients with NF2 who may not benefit from traditional hearing devices. The highest performing patients with ABIs may develop the ability to understand some speech.”
NF2 is an inherited disorder. There are two forms of the disease. In one form, patients develop growths called acoustic neuromas in both ears, which usually leads to complete deafness. A more aggressive form of the disease results in tumors throughout the brain and spine.
“Auditory brainstem implants can help restore sound perception to patients with NF2. This is critically important as a matter of safety and the ability to communicate with the world,” said Rick Friedman, MD, PhD, neurotologist. “These implants are appropriate for NF2 cases where the hearing is already lost or when the tumors have become so large that surgery is indicated and hearing preservation is not possible.”
Friedman and Schwartz make every attempt to preserve hearing in their patients. When NF2 is diagnosed with small tumors, and hearing is intact, the team will delicately remove the tumors. The team’s hearing preservation rates with the middle fossa approach are close to 80 percent. Early detection and treatment of these tumors can eliminate the need for an ABI.
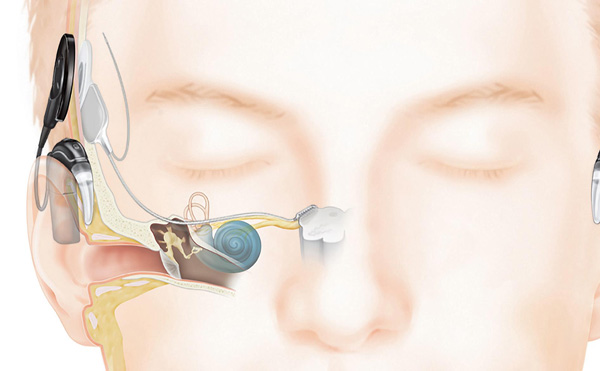
An auditory brainstem implant has two parts: a sound processor, worn behind the ear, and an implant that connects below the skin. Photo courtesy of Cochlear Americas.
An acoustic neuroma is a non-cancerous growth that represents up to 10 percent of all brain tumors. Five percent of these tumors are associated with NF2. Patients with NF2 may require surgical removal of tumors on the auditory nerve. When deafness occurs due to nerve damage, a hearing aid or cochlear implant may not be useful.
The ABI procedure is normally performed simultaneously with the removal of the auditory nerve tumor. An ABI has two parts: a sound processor, worn behind the ear, and an implant that connects below the skin. A microphone on the processor picks up noises that are converted into electrical signals that are delivered to the brain. The implant bypasses both the cochlea and the hearing nerve, taking a short cut to the brainstem. Patients over the age of 12 are eligible for this implant surgery.
After healing of the incision, the first sound processor fitting takes place. This initial stimulation session or “switch-on” is the first opportunity for the audiologist to determine if the ABI is providing hearing sensations. Using a computer, the audiologist will work with the patient to determine the most comfortable sound levels. Because the brain takes time to adapt to the electrical signals and to learn how to interpret these new sounds, several appointments are initially required. Over time, the number of visits decreases.
The ABI device is called the ABI541 System and is manufactured by Cochlear.
The UC San Diego Health Acoustic Neuroma Program specializes in the diagnosis and treatment of NF2, acoustic neuromas and complex skull base tumors. Friedman and Schwartz are internationally recognized authorities on the effective treatment of these challenging cases. Schwartz is recognized as the national leader in performing the highest volume of ABI surgeries.
Share This:
You May Also Like




Stay in the Know
Keep up with all the latest from UC San Diego. Subscribe to the newsletter today.